How many people do you know who take medications for their abdomen on a regular basis? Stomach medications for heart burn, reflux or indigestion, intestinal medications for ulcers, constipation, diarrhea, or general digestive problems. How many have had their gall bladders removed?? What if there were fibrotic adhesions from illness or injury that may have occurred years earlier? Adhesions that were impacting the performance of the abdominal organs and causing them to be symptomatic?
These tissue adhesions can be treated with physical therapy, specifically visceral therapy in which tissue mobility and motility can be restored and stomach or intestinal symptoms can be resolved which may eliminate the need for medications.
Come to Bare Necessities PT…There is Hope…True Healing Exists!!
Testimonial from my patient Tyler:
I had severe stomach problems from the age of 12 to 17. Severe pain, nausea, constipation, and diarrhea were all symptoms that I lived with on a daily basis. I missed so much school that I was unable to graduate on time. I had seen several doctors and specialists and was diagnosed with IBS, possible Crones disease and even parasites. I was prescribed several different medications and supplements, as well as changed my diet, all with little to no relief. I was told I would have to live with this for the rest of my life. I then was introduced to Tony. Just three visits cured my problem and I no longer suffer or have to worry about how I’m going to feel each day. It has changed my life. THANK YOU TONY!
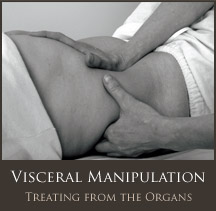
Visceral Manipulation (VM) was developed by world-renowned French Osteopath and Physical Therapist Jean-Pierre Barral. Comparative studies found Visceral Manipulation beneficial for various disorders
Digestive Disorders
Bloating and Constipation
Nausea and Acid Reflux
GERD
Swallowing Dysfunctions
Emotional Issues
Anxiety and Depression
Post-Traumatic Stress Disorder |
Pain Related to
Post-operative Scar Tissue
Post-infection Scar Tissue
Autonomic MechanismsPediatric Issues
Constipation and Gastritis
Persistent Vomiting
Vesicoureteral Reflux
Infant Colic |
VM assists functional and structural imbalances throughout the body including musculoskeletal, vascular, nervous, urogenital, respiratory, digestive and lymphatic dysfunction. It evaluates and treats the dynamics of motion and suspension in relation to organs, membranes, fascia and ligaments. VM increases proprioceptive communication within the body, thereby revitalizing a person and relieving symptoms of pain, dysfunction, and poor posture.
An integrative approach to evaluation and treatment of a patient requires assessment of the structural relationships between the viscera, and their fascial or ligamentous attachments to the musculoskeletal system. Strains in the connective tissue of the viscera can result from surgical scars, adhesions, illness, posture or injury. Tension patterns form through the fascial network deep within the body, creating a cascade of effects far from their sources for which the body will have to compensate. This creates fixed, abnormal points of tension that the body must move around, and this chronic irritation gives way to functional and structural problems.
Imagine an adhesion around the lungs. It would create a modified axis that demands abnormal accommodations from nearby body structures. For example, the adhesion could alter rib motion, which could then create imbalanced forces on the vertebral column and, with time, possibly develop a dysfunctional relationship with other structures. This scenario highlights just one of hundreds of possible ramifications of a small dysfunction – magnified by thousands of repetitions each day.
There are definite links between somatic structures, such as the muscles and joints, the sympathetic nervous system, the visceral organs, the spinal cord and the brain. For example, the sinuvertebral nerves innervate the intervertebral disks and have direct connections with the sympathetic nervous system, which innervates the visceral organs. The sinuvertebral nerves and sympathetic nervous system are linked to the spinal cord, which has connections with the brain. In this way someone with chronic pain can have irritations and facilitated areas not only in the musculoskeletal system (including joints, muscles, fascia, and disks) but also the visceral organs and their connective tissues (including the liver, stomach, gallbladder, intestines and adrenal glands), the peripheral nervous system, the sympathetic nervous system and even the spinal cord and brain.
Thanks to the dedicated work of Jean-Pierre Barral, a Physiotherapist (RPT) and Osteopath (DO), healthcare practitioners today can use the rhythmic motions of the visceral system as important therapeutic tools.
Barral’s clinical work with the viscera led to his development of a form of manual therapy that focuses on the internal organs, their environment and the potential influence on many structural and physiological dysfunctions. The term he coined for this therapy was Visceral Manipulation.
Visceral Manipulation relies on the palpation of normal and abnormal forces within the body. By using specific techniques, therapists can evaluate how abnormal forces interplay, overlap and affect the normal body forces at work. The goal is to help the body’s normal forces remove abnormal effects, whatever their sources. Those effects can be global, encompassing many areas of bodily function.
How Does Visceral Manipulation Help You?
Visceral Manipulation is used to locate and solve problems throughout the body. It encourages your own natural mechanisms to improve the functioning of your organs, dissipate the negative effects of stress, enhance mobility of the musculoskeletal system through the connective tissue attachments, and influence general metabolism. Today, a wide variety of healthcare professionals perform Visceral Manipulation. Practitioners include osteopathic physicians, allopathic physicians, doctors of chiropractic, doctors of Oriental medicine, naturopathic physicians, physical therapists, occupational therapists, massage therapists and other licensed body workers.
How is Visceral Manipulation Performed?
Visceral Manipulation is based on the specific placement of soft manual forces to encourage the normal mobility, tone and motion of the viscera and their connective tissues. These gentle manipulations can potentially improve the functioning of individual organs, the systems the organs function within, and the structural integrity of the entire body.
Harmony and health exist when motion is free and excursion is full – when motion is not labored, overexcited, depressed, or conflicting with neighboring structures and their mobility. Therapists using Visceral Manipulation assess the dynamic functional actions as well as the somatic structures that perform individual activities. They also evaluate the quality of the somatic structures and their functions in relation to an overall harmonious pattern, with motion serving as the gauge for determining quality.
Due to the delicate and often highly reactive nature of the visceral tissues, gentle force precisely directed reaps the greatest results. As with other methods of manipulation that affect the body deeply, Visceral Manipulation works only to assist the forces already at work. Because of that, trained therapists can be sure of benefiting the body rather than adding further injury or disorganization.
*from the Barral Institute



")

")
")











