Uncategorized
Socialized Medicine Impact On My PT Practice
For 20 years I practiced in Socialized Medicine as a Physical Therapist in the Army. What is the thought process of a Socialized Medicine Clinician?
….I get paid the same whether I see you for 30 visits or 3 visits…so it behooves me to heal you in as few visits as possible, so I can see the next patient and the next patient as quickly as possible. So, every skill as a clinician is aimed to heal my patients in as few visits as possible.
- In 20 years of becoming as skilled as possible at healing my patients in the fewest visits, which skills attributed to that outcome?
Manual Therapy. I average 3-4 visits from evaluation to resolution of symptoms and that’s because I put my hands on my patients. My hands tell me what systems need to be treated, my hands do the treatment and the patient’s body is able to complete the healing with typically one exercise or activity modification.
- As a socialized medicine clinician, you eliminate those aspects of your practice that don’t lend to your patients’ healing or at least don’t give you optimal bang (results) for your buck (time). What did 20 years of practice in that setting teach me was fairly useless for the time invested by myself, my staff and my patient?
- Modalities… Time and time again, studies have shown that things like ice, heat, ultrasound, electrical stimulation and use of a LASER are of very limited value to the patients’ healing. Guess what… Bare Necessities doesn’t own a single modality.
- Exercise… A lot of physical therapy practices provide a lot of supervised exercise time as it’s reimbursed well by insurance carriers and doesn’t require a lot of “work” on the part of the clinician. However, in my experience the more exercises involved in a rehab program, the less likely a patient will be inclined to do any of them once discharged, especially if they involve equipment like a stationary bike or weight machines. Once again, Bare Necessities owns no exercise equipment. Typically, I’ll prescribe at most one exercise and that exercise typically involves no equipment that a patient wouldn’t already have access to in his or her home.
- Three visits/week… When I first left the Army, I worked for a civilian clinic and it always bothered my boss that I wouldn’t schedule my patients 3 visits/week x 4 weeks. That’s how a lot of insurance based clinics operate: get the patient to commit to as many visits as possible. Part of the reason they need so many visits is that these Physical Therapy practices offer very little manual therapy and fill the time with a lot of fluff such as modalities and supervised exercise. I typically see my patients at MOST 1 visit/week and the course of care is usually complete sometime around the 3-4 visit range around the 6-8th
I’m not blaming civilian physical therapists for their practice philosophy. they are practicing as they were trained and to some extent doing what they need to do to survive with a very poor insurance industry reimbursement rate.
Lastly, in a medical setting with the foundation of healing the patient in as few visits as possible. I was blessed to receive the Surgeon General’s award for clinical expertise as best of the best, an award that was given to the top 4-5% of military clinicians. Come to Bare Necessities…it’s physical therapy like you have never experienced before. There is hope for healing!!

Palpate: Pal-pate
pal-pat-ed, pal-pat-ing, pal-pates
To examine by feeling with hands and fingers; used by some archaic physical therapists, who (Bless their Hearts) just don’t know any better.

As many of you know, I’m currently fortunate enough to be on an APTA board tasked with developing a definition for a new Board Certification which will fall along the lines of: Primary Care or Family Practice or Family Health (or whatever title meets consensus). Well as we flushed out what exam skills should be included in this specialty we fleshed out a solid 2-3 paragraphs on behavioral testing and under palpation? Nothing. The Palpate bullet stood alone. When I suggested it needed some description the other members of the group (all senior and experienced clinicians) didn’t show a lot of excitement to elaborate on the “palpation” bullet.
A little about me….my exam is MOSTLY palpation…the more experienced I become as a clinician the MORE I rely on palpation. I was an Army Physical Therapist for 20 years and I was awarded the Surgeon General’s award for clinical expertise. In one year of a cash-based clinical practice with 0$ spent on advertising I had a 4-week waiting list. I’m only mentioning this to underscore that I must be doing something right as a clinician and palpation is the cornerstone of my practice.
I always tell my students that “your eyes can be fooled, your ears misled, but your hands will perceive a true reflection of what is happening in your patient’s body.” If my clinical experience has any validity to it at all…and I’m inclined to believe it does based on my patient success rate…then why has the profession of physical therapy turned away from palpation? I feel that as the pendulum has swung towards Evidence Based Practice, it has at the same time swung away from Intuition and Feeling of which palpation is a tool. Our research based institutions have a hard time “measuring” palpation for validity or reliability and so it’s been shunned to a great extent.
I’m not arrogant or foolish enough to think that the ramblings of an “old” clinician will affect any change of teaching in any physical therapy program, I’m just mentioning it here to plant the seed for younger clinicians. These younger clinicians who at some point in their career may become “burned out” or disillusioned with their profession because patient after patient just doesn’t seem to be making spectacular improvement in spite of following the Clinical Practice Guidelines to the letter. I’d advise these younger clinicians to take a moment…close their eyes, screen their ears, turn ON their intuition and really “feel” what their hands and fingers are palpating.
Shin Splints

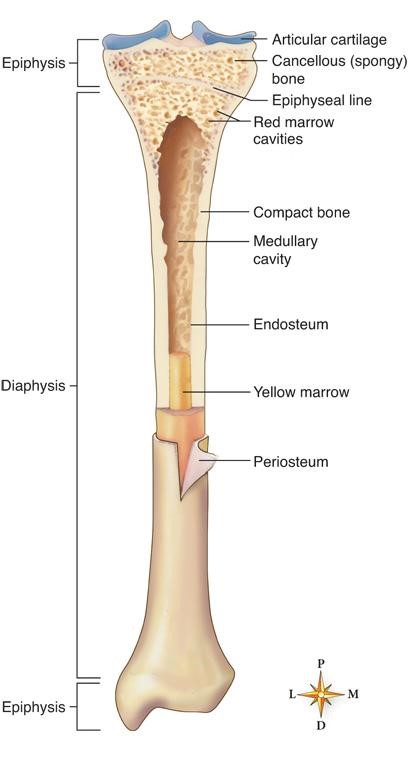
The most common cause of shin splint pain is excessive (in magnitude or duration) of tension on the tibia by the Posterior Tibialis muscle. The reason the pain is so extreme is that the Posterior Tibialis muscle fibers blend with the skin of the Tibia which is called the periosteum. The periosteum has the majority of all sensory nerve endings in the entire bone…so if you are having shin splints, you are having “bone pain” as if the periosteum is tearing…that can be excruciating
Once you understand the job of the Posterior Tibialis you will understand why it hurts and how to facilitate healing. When you walk or run the arch on the inside of your foot lowers with shock absorption impact in a motion termed pronation

The Posterior Tibialis resists this pronation motion much like a shock on a car. So, the more the foot and leg roll inward in both the magnitude and duration…the more “work” demands are placed on the Posterior Tibialis as it resists this collapse of the inside of your foot. The more the Posterior Tibialis works, the more it pulls on the periosteum and the more likely you will have shin pain.
Treatment for Posterior Tibial Shin pain.
- Ice will work as an analgesic…it treats the pain, but doesn’t address the pathology.
- Heat is also an analgesic…it treats the pain, but it may improve circulation to the injured tissue which can bring nutrients needed for healing.
- Anti-inflammatories. They also work as an analgesic and if taken as prescribed will in time reduce inflammation, so once again they do not address the actual pathology.
- Reducing the demand on Tibialis Posterior will lead to true healing of the pathology. Rest can come in several magnitudes…
- Reduce pronation… limit wearing shoes that offer little or no support to the inside of your feet and time walking barefoot.
- Reduce pronation… limit walking on unstable surfaces like sand or gravel.
- Reduce pronation… you can purchase shoes that offer a higher level of motion control and any reputable running shoe store can help you select those.
- Reduce pronation… you can add an arch support to further limit pronation. Feel free to come to Bare Necessities for a free gait analysis to give you advice on both shoe and potential arch support prescription…if you don’t live near Laramie, WY…we are still happy to give you free advice if you can send us video of you walking barefoot on a treadmill. Email to Tony@BarePT.com or send larger files to Anthony.Bare on facebook.
- Reduce Impact… decrease minutes of running or walking. Consider non-impact activities like biking and swimming.
- Reduce Impact… do your walking or running on a treadmill. A good treadmill provides a level and supportive surface.
- Reduce Impact… Reduce running downhill and consider increasing running uphill (once again made easier on a treadmill).
- There is no significant role for strengthening for this pathology… Tibialis Posterior is already over worked…more work is not the answer.
- There is no significant role for stretching for this pathology… the Tibialis Posterior is as tight as it “needs” to be to do it’s job.
- Manual therapy. There is a role for manual therapy to facilitate healing of the Tibialis Posterior and the Tibial periosteum, but if you haven’t addressed #4 above the manual therapy will be much less effective.
While Tibialis Posterior is the most common cause of shin pain, there are other causes and if your symptoms aren’t located on the lower inside of your shin or your pain doesn’t rapidly respond to the treatments suggested above, then it is time to seek medical evaluation.
The Fallacy of Leg Length Correction
")

For many years I was honored to be the Military’s expert in lower extremity biomechanics and I’ve made tens of thousands of orthotics in my career and yet I’ve only added a leg length correction in maybe 10-20 instances. The reason this came to mind is that I recently assessed a patient s/p TKA who became one of the very rare patients to add her name to that list. I thought I would share my thoughts on the subject because I certainly have run into no shortage of patients (and providers) who strongly believe in correcting for leg length difference.
- Since Jesus ascended to heaven there hasn’t been another person on the planet whose legs are symmetrical and really how could we be symmetrical? The obvious is the actual length of the femur and tibia, but functional leg length difference is more often due to asymmetry of Coxa, femoral, genu, and tibial varus/valgus alignment
")
")
2. Leg length asymmetry is just one part of the picture of frontal plane function…the real culprit is often what’s happening below the ankle and understanding those biomechanics will help you go a long way to deciphering the potential effect of leg length difference on functional biomechanics.
3. The body has numerous mechanisms to cope or compensate for frontal plane deviations and typically it’s been coping well for years or decades.

How do I decide whether or not to correct for a leg length asymmetry?
- Has something changed in the bone? Most of my leg length corrections followed a TKA, THA, or Femur/Tibial fracture. Some change in bone length that the patient’s body hasn’t lived with for decades.
- Is there an observable frontal plane gait deviation? Look for a drop in the pelvis on one side that would indicate an uncompensated leg length difference that might need intervention.
- Does the patient present with chronic or recurrent frontal plane pathology? Unilateral sacroiliac/trochanteric symptoms (bursitis, piriformis, etc), lateral thigh/knee pain (ITB, Vastus Lateralis, and patellofemoral pain).
- You’ve balanced the frontal plane issues below the ankle (typically: rearfoot varus, forefoot varus, and/or unstable midtarsal joint) and the patient’s symptoms have not improved. The foot has so much more leverage to impact the pelvis, you will be amazed how quickly your posterior and lateral hip pain patients recover when you address frontal plane issues below the ankle.
So you might be asking, why not correct for the apparent leg length asymmetry? What’s to lose?
- As noted above, of all the things that could lend to the appearance of a leg length difference, most of them are more variations of angulation (varus or valgus) than a true difference in length of either the femur or tibia (unless something has changed in the bone, see #1 above).
- You might actually be creating a leg length asymmetry. (Whatever the patient has going on, they may have been coping well with it for decades and changing that may cause more problems than it improves).
- Correcting for a leg length difference inside the shoe can significantly change the fit of a shoe far more than treating the frontal plane issues in angulation below the ankle…and if the patient doesn’t like how his/her shoe is fitting, she won’t wear the correction. Typically the most correction you can fit inside a shoe before shoe fit becomes an issue is ¼”, so the picture below is for your entertainment purposes. I was stationed at Brooke Army Medical Center in 1998 when I ordered a “custom shoe modification” for a 2” leg length difference secondary to femur fracture and instead of doing the hard work of adding the correction to the sole of my patient’s shoe, the Orthotist did the ridiculous work of constructing the biggest heel lift I’ve ever seen. I’ve kept it as a souvenir.

Postpartum Journal of a Manual Therapist
- Prenatal: There is a whole blog written about Amy’s first two births, but I’ll summarize. Graham was a traumatic inverted “T” C-section and Stella was a home birth VBAC (Vaginal birth after C-section). Both Graham and Stella were well past 41 weeks gestation and over 40 hours of hard labor and 4 hours of pushing during the VBAC birth. I treated Amy’s c-section scar and uterus extensively before conception and during the final trimester I did several sacrotuberous and sacrospinous ligament releases. Juliet was born at 39 weeks 6 days after only 5-6 hours of active labor and less than 20 minutes of pushing. I’m not claiming responsibility for the vastly easier birth, but as a manual therapist it sure makes sense that I contributed. From Amy: I feel like the work that Tony did prenatally made a huge difference. Juliet also engaged in my pelvis prior to labor which was a first for me. My first two births were difficult due to baby’s potitioning and presentation. The assumption (by several medical and birth professionals) is that I had soft tissue restrictions in my pelvis and also scar tissue that prevented optimal fetal positioning and vaginal birth or easy vaginal birth. Having my husband treat both the soft pelvis and scar tissue allowed the baby to get into my pelvis properly and to rotate and descend more easily in labor. As a former doula I have extensive knowledge in optimal fetal positioning, I made it a point to learn as much as I could after my own experiences and I have a great understanding of how the pelvis and baby work during birth. I actually did less to prepare for my third baby than I did my second one as far as optimal fetal positioning techniques are concerned, the biggest difference was the body work that my husband did. One thing that I really appreciated was that Tony and I could speak the same language when discussing the pelvis concerning pregnancy and birth and then he was able to take it farther with his visceral treatment knowledge.
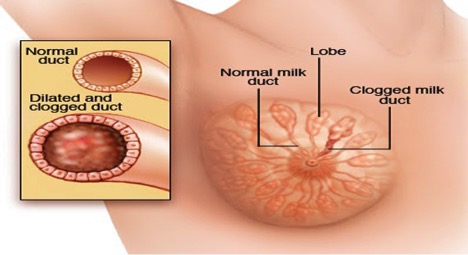
- Mastitis: Amy started running a fever a few days after birth and sure enough I palpated a rigid quadrant in her right breast. I treated the area 5 times over the next 2 days and combined with Ibuprofen, ice packs and cabbage leaf compresses she had complete resolution of her symptoms in 48 hours without having to drag Juliet and herself to the acute care clinic for antibiotics. From Amy: On the 3rd day postpartum I started feeling feverish and having chills. I didn’t notice any hardness or swelling in my breast right away but when Tony palpated he felt the blockage and soon it was hard, engorged, red, warm and very painful. I felt as though I had the flu. We gave ourselves a deadline of 48 hours for improvement or we’d go in. After Tony treated my breast the first time I could tell it was better. The pain was less and it was less engorged. Treatment the first time was pretty painful but each time after it felt better. By our 48 hour deadline it was as if I had never had mastitis at all. My fever peaked at 102.7 (while taking Tylenol) but I was able to stop taking Tylenol completely and it didn’t return. The engorgement and redness was gone and there was no pain. I took ibuprofen for an additional 24 hours.
- Uterinitis: I’m not sure what her diagnosis would have been, but her symptoms included a deep pressure and fullness and a “prolapse” sensation along with feeling “crampy”. On palpation I could definitely appreciate the fullness of the uterus which I treated using visceral therapy techniques with resolution of all symptoms following one treatment. Amy: The only way I could describe what I was feeling was to use the word prolapse. It just felt heavy and full in my lower abdomen and even in the top of my vagina. I did look “down there” to see if I could see anything since sometimes prolapse after birth can happen and it can be bad enough for the cervix or even uterus to fall into the vagina but I’m happy to report that at 2 weeks postpartum I looked completely normal and pre-baby in the lady area. I didn’t tear during the birth and really had very little swelling so healing was fast externally but I was really glad to see nothing coming out either. I’ve been doing a ton of kegels every day but after the first time Tony treated my uterus that heavy feeling went away. I did pass some small clots after that treatment but my bleeding is pretty minimal and after the second treatment I had no more clots. I didn’t really want to talk to him about this issue, I am still his wife and want to maintain some level of sexuality and since he had already watched me push the baby out I didn’t want to become “clinical” to him but I realized if I were going to talk to anyone about it, it should be him. He was the most likely to help me and he did. I’m still not 100% sure that I don’t have some prolapse. My pelvic floor is pretty weak and even before this pregnancy I had a lot of incontinence when I sneezed and especially when I run. I still want to do some pelvic floor rehab with a PT that specializes in it but I want to continue to have my husband treat me externally until I start going.
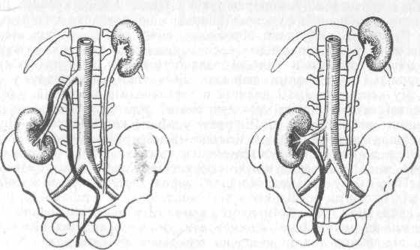
- Kidney Ptosis: Amy developed left flank pain which was worse when laying supine, with change of positions and breathing. I examined and did some treatment on her ribs, but they really felt fine. When I palpated her left kidney her symptoms were aggravated. The left kidney certainly makes sense for two reasons… 1.) In late term pregnancy the baby spends most of her time on the left side of her mom’s body 2.) There is a genitourinary vein that drains the uterus and ovaries to the left kidney that isn’t duplicated on the right side. This extra fascial structure would tend to drag the kidney inferiorly once the uterus retreats that direction after birth. I treated Amy’s kidney using visceral therapy and had complete resolution of her symptoms in one treatment. Amy: I had sharp shooting pains in my back that had me doubled over and in tears. I thought I’d broken a rib but I had done nothing to injure myself. The pain was so bad that I might have actually gone in for drugs but instead we got up and Tony treated me at 2am. It immediately felt better and I went from not being able to lay down comfortably to being able to go asleep. The next day it was a bit sore and the next day 100% better. This was about the time I started thinking my husband was a miracle worker. It’s not the first time I or someone else has thought that though.
- Sigmoid dysfunction/constipation: Amy was having unusual pain and difficulty with bowel movements and on palpation the sigmoid colon was clearly the culprit. Once again complete resolution of symptoms following one visceral therapy treatment. Amy: This is another one that I didn’t want to talk about. I don’t like “potty talk” and pretty much avoid that topic with my husband but after two weeks of pretty intense bathroom pain I had to say something. I also felt like I couldn’t talk about the uterine stuff without mentioning this. Basically, every time I had been to the bathroom since I had the baby was super painful. If you’ve ever had a vaginal birth you know that first time going is pretty scary but it didn’t stop being scary. It got more scary because I knew it would hurt. Simple gas hurt. Laying on my back hurt. After two weeks I finally spoke up and things were better the next day after one treatment. He said my colon felt “ropey”. I’m happy to report that all is well and I don’t have to talk about it any more!
Why mention all this? I truly believe that moms are mostly expected to suffer through pregnancy and postpartum pains and difficulties as all part of “being a mom”. Pain and dysfunction are NOT natural states for the human body and I’m a firm believer in giving it a shot manual-therapy-wise. If you are a mom or know a mom recently postpartum, ask her how she’s doing. You may be able to alleviate so much of her pain and birth related difficulties. Trust your hands! Amy: I do think he’s right that as moms we are just expected to have pain and suffer through it. We don’t have to. There’s so much that can be treated and that can feel better.
Lastly, if you are one of those therapists who doesn’t believe in visceral therapy, please contact me! If you are open to the possibility, please attend a course and your practice will never be the same again and you will be able to help so many more people!!
The Fallacy of Calf Stretching
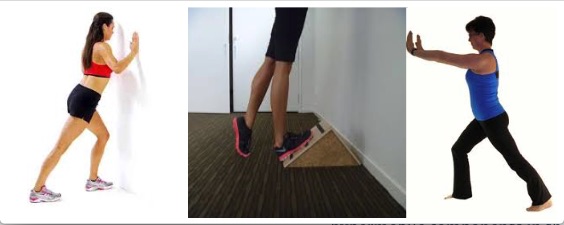
For decades physical therapists and physicians have been instructing their patients to stretch their calves for ALL manner of foot pain, heel pain, Achilles tendonitis, ankle pain and calf pain.
What if I told you that the underlying etiology of just about all musculoskeletal foot, ankle and leg pain is hypermobility (over flexible)?
You might reply, “But when I stretch I can feel how tight it is.”
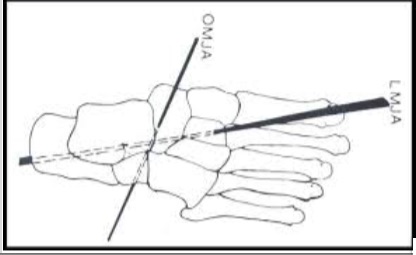
I would counter with, “It’s tight because of an instability elsewhere in the foot-ankle-leg complex…which you are arguably making worse by stretching it.” EVEN THOUGH IT CAN FEEL BETTER SHORT-TERM following stretching. The most common place for hypermobility in the foot-ankle-leg structure is the oblique axis of the midtarsal joint. Every time you walk it is common to bend your foot at this joint instead of at your ankle joint…so the ankle joint/calf is stiff because your body does not make it move in normal gait.
When you stretch your calf, you are actually stretching everything on the bottom of your foot to the back of your knee. Those structures already hypermobile stretch first and most easily, then the structures that have normal flexibility and if you continue to stretch you will gradually make gains in the most “stiff” structures in the chain….but not until you’ve already stretched PLENTY of stuff that did not need it.
Yes, I’ll admit you will gain motion temporarily in the most “stiff” structures, but you won’t retain it, because your body will just continue to bend through the hypermobile joint because it’s easier. The underlying issue is INSTABILITY…you should just about NEVER stretch an unstable joint. You heal the stiffness in the calf, by stabilizing the foot.
How to stabilize the midtarsal joint…
TAPING: In my clinical experience, there has NEVER been a foot pain that didn’t feel better with a low-dye tape job. This rigid athletic tape application stabilizes the hypermobile components in the chain and the whole system feels better when stabilized…not when stretched. There are about a dozen elastic tape options as well.

STRENGTHENING: There is really no external lower extremity muscle that stabilizes the oblique axis of the midtarsal joint…so calf exercises and theraband exercises are fairly useless. There is value in strengthening the intrinsics, so proprioceptive exercises are very useful if symptoms allow.
ORTHOTICS: Arch supports custom and otherwise are of very limited value as they push up into the longitudinal axis of the midtarsal joint and if anything push the Center of Pressure laterally to the already unstable oblique axis. However, custom orthotics designed to specifically stabilize the oblique axis of the midtarsal joint will have a dramatic and immediate impact. If you have any questions about how to order this type of orthotic, please email me at Tony@BarePT.com or visit my webpage at BarePhysicalTherapy.com.
House Slippers for Orthortics
Friends, Amy found a house slipper that works perfectly with orthotics. You can put an orthotic in the slipper or I can put a permanent modification in the slippers for you. With winter coming we needed a good solution for hard floors, cold feet and wearing an orthotic because if you are like Amy, she needs that support when she’s home as much as when she’s not.
The brand is TOMS and the insole that comes with them easily comes out.




TOMS can be found easily online, just Google search it or at Journey’s, Nordstrom Rack and Dillard’s locally.
If you prefer to have the permanent modification the cost is $50 for one pair of slippers/shoes or $90 for two pair. You can also put your existing orthotics in them if you want to swap them out with your other shoes or you can order an extra pair for $85 to use exclusively in the slippers.
Why the Affordable Care Act can do Nothing to Improve Health Care
- The problem is not access. For the vast majority of Americans, access to health care isn’t the issue. The issue is quality of care. Because the average quality of care is so poor in American medical offices, few patients are accurately diagnosed and fewer still are healed. Typically, at best they have their symptoms managed. Why is quality of care so poor?
- `Medical appointments are too short. The insurance industry reimburses so poorly that the typical primary care appointment is less than 10 minutes long. In my profession you are lucky to have 25-30 minutes of face-to-face time with your physical therapist. The insurance industry documentation requirements for reimbursement leads to more and more mouse clicking and “key phrase” typing which steals more minutes from actual patient interaction. The vast majority of documentation requirements lend little/no value to the patient interaction or even to follow-on care appointments.
- Medical professional skill level. Fewer and fewer medical appointments are conducted by actual physicians. More and more care is provided by physician extenders (Physician Assistants and Nurse Practitioners) and ancillary medical professionals (CNA’s and MA’s). These medical assistants to physicians are doing their best, but they have less training, less time and more documentation requirements. The deck is stacked against them. I’m a firm believer in direct access for physical therapists for musculoskeletal pain. We have more training and evaluation appointment time than any PCP (Primary Care Provider and if anything, insurance companies should mandate that their beneficiaries be required to see a physical therapist BEFORE seeing a PCP. Physical Therapists are more qualified to make follow on consultations and radiographic orders (X-rays, CT scans, MRI’s, etc). This system has already been in place and extremely successful in all branches of the U.S. military.
- Quantity: Number of trained medical professionals. Our profession has a vast shortage of trained medical professionals and I’ve said many times that if the government wants to get involved improving healthcare it should create more scholarship opportunities for Americans to attend various medical schools (ranked based on need assessments). I’m also a firm believer in reinstating a medical internship program. Right now if you have all the intangibles to be the best physician in the history of the United States, but can’t pass the MCAT, you will never enter the profession. I believe that with a 3-5 year internship interspersed with select college course work, writing assignments and a LOT of 1:1 mentorship by experienced clinicians (>10 years in field), that we would be able to field another group of highly skilled medical professionals who would improve both quality and quantity deficits.
2. Little to no focus on prevention. There is no money to be made in the field of prevention, all the money is in pharmaceuticals and surgery once illness or injury has progressed. I’m sure you don’t have to believe in conspiracy theories to imagine the big pharmaceutical companies might be lining the pockets of politicians and government employees to allow the status quo. This is far from my area of expertise, but imagine the effect of pollution, pesticides, “food” additives, fertilizers, artificial food dyes, artificial sweeteners…many of the above are banned in some or all of other modern countries, but not the United States. Don’t underestimate the effect of a stationary lifestyle where Americans sit far too much hunched over a laptop or cell phone. What if insurance companies rewarded fitness with cash rebates to their beneficiaries? What if our government rewarded agriculture and food industry for producing “clean” food? What if insurance companies rewarded individual practitioners for best results and healing rates?
If the average American were healthier he/she would need fewer appointments and access to healthcare and cost of medical care would both improve.
Visceral Therapy for stomach problems
How many people do you know who take medications for their abdomen on a regular basis? Stomach medications for heart burn, reflux or indigestion, intestinal medications for ulcers, constipation, diarrhea, or general digestive problems. How many have had their gall bladders removed?? What if there were fibrotic adhesions from illness or injury that may have occurred years earlier? Adhesions that were impacting the performance of the abdominal organs and causing them to be symptomatic?
These tissue adhesions can be treated with physical therapy, specifically visceral therapy in which tissue mobility and motility can be restored and stomach or intestinal symptoms can be resolved which may eliminate the need for medications.
Come to Bare Necessities PT…There is Hope…True Healing Exists!!
Testimonial from my patient Tyler:
I had severe stomach problems from the age of 12 to 17. Severe pain, nausea, constipation, and diarrhea were all symptoms that I lived with on a daily basis. I missed so much school that I was unable to graduate on time. I had seen several doctors and specialists and was diagnosed with IBS, possible Crones disease and even parasites. I was prescribed several different medications and supplements, as well as changed my diet, all with little to no relief. I was told I would have to live with this for the rest of my life. I then was introduced to Tony. Just three visits cured my problem and I no longer suffer or have to worry about how I’m going to feel each day. It has changed my life. THANK YOU TONY!
The Therapeutic Value of Visceral Manipulation
Visceral Manipulation (VM) was developed by world-renowned French Osteopath and Physical Therapist Jean-Pierre Barral. Comparative studies found Visceral Manipulation beneficial for various disorders
| Digestive Disorders Bloating and Constipation Nausea and Acid Reflux GERD Swallowing Dysfunctions Emotional Issues |
Pain Related to Post-operative Scar Tissue Post-infection Scar Tissue Autonomic MechanismsPediatric Issues Constipation and Gastritis Persistent Vomiting Vesicoureteral Reflux Infant Colic |
VM assists functional and structural imbalances throughout the body including musculoskeletal, vascular, nervous, urogenital, respiratory, digestive and lymphatic dysfunction. It evaluates and treats the dynamics of motion and suspension in relation to organs, membranes, fascia and ligaments. VM increases proprioceptive communication within the body, thereby revitalizing a person and relieving symptoms of pain, dysfunction, and poor posture.
An integrative approach to evaluation and treatment of a patient requires assessment of the structural relationships between the viscera, and their fascial or ligamentous attachments to the musculoskeletal system. Strains in the connective tissue of the viscera can result from surgical scars, adhesions, illness, posture or injury. Tension patterns form through the fascial network deep within the body, creating a cascade of effects far from their sources for which the body will have to compensate. This creates fixed, abnormal points of tension that the body must move around, and this chronic irritation gives way to functional and structural problems.
Imagine an adhesion around the lungs. It would create a modified axis that demands abnormal accommodations from nearby body structures. For example, the adhesion could alter rib motion, which could then create imbalanced forces on the vertebral column and, with time, possibly develop a dysfunctional relationship with other structures. This scenario highlights just one of hundreds of possible ramifications of a small dysfunction – magnified by thousands of repetitions each day.
There are definite links between somatic structures, such as the muscles and joints, the sympathetic nervous system, the visceral organs, the spinal cord and the brain. For example, the sinuvertebral nerves innervate the intervertebral disks and have direct connections with the sympathetic nervous system, which innervates the visceral organs. The sinuvertebral nerves and sympathetic nervous system are linked to the spinal cord, which has connections with the brain. In this way someone with chronic pain can have irritations and facilitated areas not only in the musculoskeletal system (including joints, muscles, fascia, and disks) but also the visceral organs and their connective tissues (including the liver, stomach, gallbladder, intestines and adrenal glands), the peripheral nervous system, the sympathetic nervous system and even the spinal cord and brain.
Thanks to the dedicated work of Jean-Pierre Barral, a Physiotherapist (RPT) and Osteopath (DO), healthcare practitioners today can use the rhythmic motions of the visceral system as important therapeutic tools.
Barral’s clinical work with the viscera led to his development of a form of manual therapy that focuses on the internal organs, their environment and the potential influence on many structural and physiological dysfunctions. The term he coined for this therapy was Visceral Manipulation.
Visceral Manipulation relies on the palpation of normal and abnormal forces within the body. By using specific techniques, therapists can evaluate how abnormal forces interplay, overlap and affect the normal body forces at work. The goal is to help the body’s normal forces remove abnormal effects, whatever their sources. Those effects can be global, encompassing many areas of bodily function.
How Does Visceral Manipulation Help You?
Visceral Manipulation is used to locate and solve problems throughout the body. It encourages your own natural mechanisms to improve the functioning of your organs, dissipate the negative effects of stress, enhance mobility of the musculoskeletal system through the connective tissue attachments, and influence general metabolism. Today, a wide variety of healthcare professionals perform Visceral Manipulation. Practitioners include osteopathic physicians, allopathic physicians, doctors of chiropractic, doctors of Oriental medicine, naturopathic physicians, physical therapists, occupational therapists, massage therapists and other licensed body workers.
How is Visceral Manipulation Performed?
Visceral Manipulation is based on the specific placement of soft manual forces to encourage the normal mobility, tone and motion of the viscera and their connective tissues. These gentle manipulations can potentially improve the functioning of individual organs, the systems the organs function within, and the structural integrity of the entire body.
Harmony and health exist when motion is free and excursion is full – when motion is not labored, overexcited, depressed, or conflicting with neighboring structures and their mobility. Therapists using Visceral Manipulation assess the dynamic functional actions as well as the somatic structures that perform individual activities. They also evaluate the quality of the somatic structures and their functions in relation to an overall harmonious pattern, with motion serving as the gauge for determining quality.
Due to the delicate and often highly reactive nature of the visceral tissues, gentle force precisely directed reaps the greatest results. As with other methods of manipulation that affect the body deeply, Visceral Manipulation works only to assist the forces already at work. Because of that, trained therapists can be sure of benefiting the body rather than adding further injury or disorganization.
*from the Barral Institute
